For a child to keep confident in the medical staff, it is essential to suppress pain during the various treatments performed on him. Today, it is possible.
A child may not suffer, but say the opposite because he is afraid. Fear is a form of trauma and must be taken into account in the management of pain. There are ways to make it disappear.
Pain free procedures are now widely spread in all hospitals. Professionals and parents should ensure their application.
Children with ataxia telangiectasia are brought to be often confronted with the medical community, synonymous for great anxitety. In order that visits to doctors or in hospitals become a routine, preferably nice, it is essential that all the care they receive is surrounded by maximum precautions. To do this, one must:
- create as much as possible a pleasant environment around the child
- establish a trusting relationship with him
- suppress pain in medical procedures
Confidence
In fact, these last two points are closely related. You can not tell a child: "Trust me" if afterwards, he is suffering. This is obviously relevant to the medical staff, but it is equally important for parents who bring, in spite of themselves, their child to the hospital. If the place is synonymous with pain, then the child may not trust them anymore.
Generally speaking, it is a truism to say that confidence is established if the words are followed by actions. In other words, each medical act has to be explained to a child: how it will be done and what means will be used so that he won't feel anything ... and do what was said.
Injections
When we think "hospital," we usually think "injection".
With the prospect of the injection comes into play a series of worrying criteria such as the size of the syringe or the virtuosity of the nurse. In fact, we can reduce the number of objective criteria for pain to four:
-
the spot where the injection is going to be: it may be more or less dense in pain sensors, therefore more or less sensitive
-
the softness of the contact made with the nursing staff: this will determine the degree of confidence that the child is going to give prior to anything
-
the immediate environment: for example, the dispersion of attention, by singing a song or watching a cartoon... is likely to lower the anxiety preceeding the injection
-
the diameter of the needle: it is variable and determines more or less the means used to reduce pain:

-
needles for subcutaneous injections (vaccines, local anesthesia, immunoglobulins ...) are very thin and just cause a slight tingling sensation at the time of the act. This tingling can be completely removed by applying a local anesthetic cream or a patch, between 1 and 4 hours before (EMLA cream or patch in).
-
blood tests and infusions needles are slightly larger and the act itself is a bit more complicated because the nurse must find and pierce a vein, which can be both impressive and painful for the patient, not to mention the risk of failure. But again, the anesthetic cream mentioned above works miracles. In order to de-stress everyone, including parents and nurses, it is also possible to use a sedative and euphoric gas, a harmless mixture of nitrous oxide and oxygen (Entonox, Kalinox,...)
-
for even larger needles, like those used for amniocentesis or puncture, local anesthesia is used with previous sedative injections, which brings us back to the two previous cases, thus making the act also painless.
Surgeries
The recommended precautions below are valid mainly for surgery requiring only local anesthesia, a skin biopsy in dermatology for example. It is a deep skin sample, which can be impressive and painful if not properly prepared, if all precautions are not taken to minimize the inconvenience. But they also apply to preparations to more invasive acts or general anesthesia.
Thus, it is desirable that the following conditions are met, in addition to environmental criteria and confidence as previously treated:
- The act has to be conducted at the hospital in the presence of at least two nurses in addition to the doctor: one to care for the child, the other one to attend the doctor.
- Before the start of the operation, a sedative, sometimes the Entonox (see above), should be administered to the child so that he does not care what happens around him, that he does not see the instruments that will be used or even the doctor performing the act on him.
- The time of action of the anesthetic used must be scrupulously respected.
If these three conditions are met, then your child will not feel anything. He probably will not remember anything. This will allow to tackle the following acts with great serenity.
This protocol is the only one to respect the anti-pain charters that are now well established in modern medicine.
You have the inalienable right to refuse or to halt an operation that does not comply with these conditions.
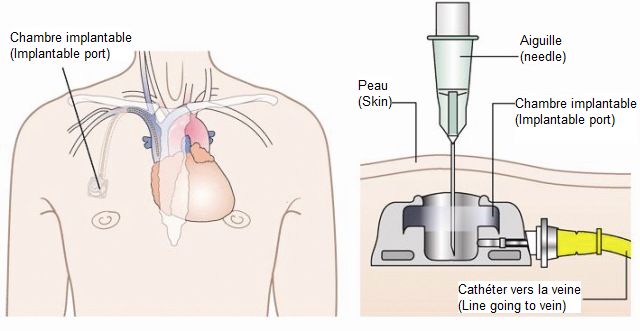
IMPLANTED INJECTION CHAMBERS OR PAC (Port-A-Cath)
Patients who require regular infusions as the injection of immunoglobulins may see their venous capital deteriorate over time (veins difficult to penetrate, damaged by the products of injections ...), making the infusion difficult, so painful, to set.
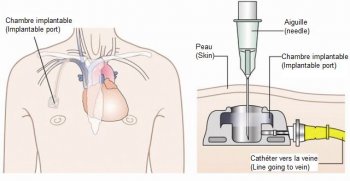 One solution is to put, under general or local anesthesia, a small injection chamber under the skin, usually over the pectoral muscle next to the clavicle. Also known as Porth-a-Cath (PAC), it is equipped with a catheter which is connected to a large vein near the heart. The chamber is closed by a silicone membrane to receive a needle for injection or allow blood sampling. The needles used are specific (Huber tip or Gripper System) and must be positioned with all the precautions of sterility.
One solution is to put, under general or local anesthesia, a small injection chamber under the skin, usually over the pectoral muscle next to the clavicle. Also known as Porth-a-Cath (PAC), it is equipped with a catheter which is connected to a large vein near the heart. The chamber is closed by a silicone membrane to receive a needle for injection or allow blood sampling. The needles used are specific (Huber tip or Gripper System) and must be positioned with all the precautions of sterility.
This system may present some risks, however rare if used properly and with precaution:
- risk of infection: mostly due to neglect of sterility, especially after implantation
- risk of clogging of the catheter: it is called a thrombosis and can be prevented by rinsing thoroughly before and after injection
- risk of turning over: usually due to bad manipulation
- risk of embolism: a consequence to thrombosis or manipulation of the chamber without care
A final drawback of the system is purely aesthetic: the PAC may appear under the skin and form a small ball.
However, it has significant advantages: :
- it avoids damage to the veins
- It offers great comfort of use by:
- suppressing pain of the injection only by using a local anesthetic cream (EMLA)
- suppressing pain usually caused by searching for a vein with the needle
- reassuring both patients and their families as well as caregivers to the extent that the medical procedure is repeated each time the same way with the certainty of the absence of pain
Anyway, the decision to implement a PAC has to be discussed with the doctor.

 Parents know their child best and guide the doctors who have to listen. By reporting a change in behavior, fatigue, decreased appetite, lymph node, an allergic reaction., etc ..., they give them vital information. It is therefore important to pay attention to any changes in the child with Ataxia telangiectasia, whether physical or behavioral, or if they appear after a change in treatment.
Parents know their child best and guide the doctors who have to listen. By reporting a change in behavior, fatigue, decreased appetite, lymph node, an allergic reaction., etc ..., they give them vital information. It is therefore important to pay attention to any changes in the child with Ataxia telangiectasia, whether physical or behavioral, or if they appear after a change in treatment.